
Ryzodeg FlexTouch (1pc)
Inhouse product
-
 ৳1,030.00
৳1,030.00৳1,550.00 -
৳250.00
৳500.00 -
৳110.00
৳150.00 -
৳12.00
৳15.00 -
৳775.60
৳1,108.00 -
৳130.00
৳135.00





Reviews & Ratings
One pre-filled pen contains 300 units of insulin degludec/insulin aspart in 3 ml solution.
*Produced in Saccharomyces cerevisiae by recombinant DNA technology.
Excipients/Inactive Ingredients: Glycerol, metacresol, phenol, sodium chloride, zinc acetate, hydrochloric acid/sodium hydroxide (for pH adjustment) and water for injections.
Pharmacology: Pharmacodynamics: Mechanism of action: Insulin degludec and insulin aspart bind specifically to the human insulin receptor and result in the same pharmacological effects as human insulin. The blood glucose-lowering effect of insulin is due to the facilitated uptake of glucose following the binding of insulin to receptors on muscle and fat cells and to the simultaneous inhibition of glucose output from the liver.
Pharmacodynamic effects: The pharmacodynamic effect of Ryzodeg is distinctively separated for the two components (figure), and the resulting action profile reflects the individual components, the rapid-acting insulin aspart and the basal component insulin degludec.
The basal component of Ryzodeg (insulin degludec) forms soluble multi-hexamers upon subcutaneous injection, resulting in a depot from which insulin degludec is continuously and slowly absorbed into the circulation leading to a flat and stable glucose-lowering effect. This effect is maintained in the co-formulation with insulin aspart and does not interfere with the rapid-acting insulin aspart monomers.
Ryzodeg has a rapid onset of action occurring soon after injection providing mealtime coverage while the basal component has a flat and stable action profile providing continuous coverage of the basal insulin requirements. The duration of action of a single-dose of Ryzodeg is beyond 24 hours. (See figure.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe total and maximum glucose-lowering effects of Ryzodeg increase linearly with increasing doses. Steady state will occur after 2-3 days of dose administration.
There is no difference in the pharmacodynamic effect of Ryzodeg between elderly and younger patients.
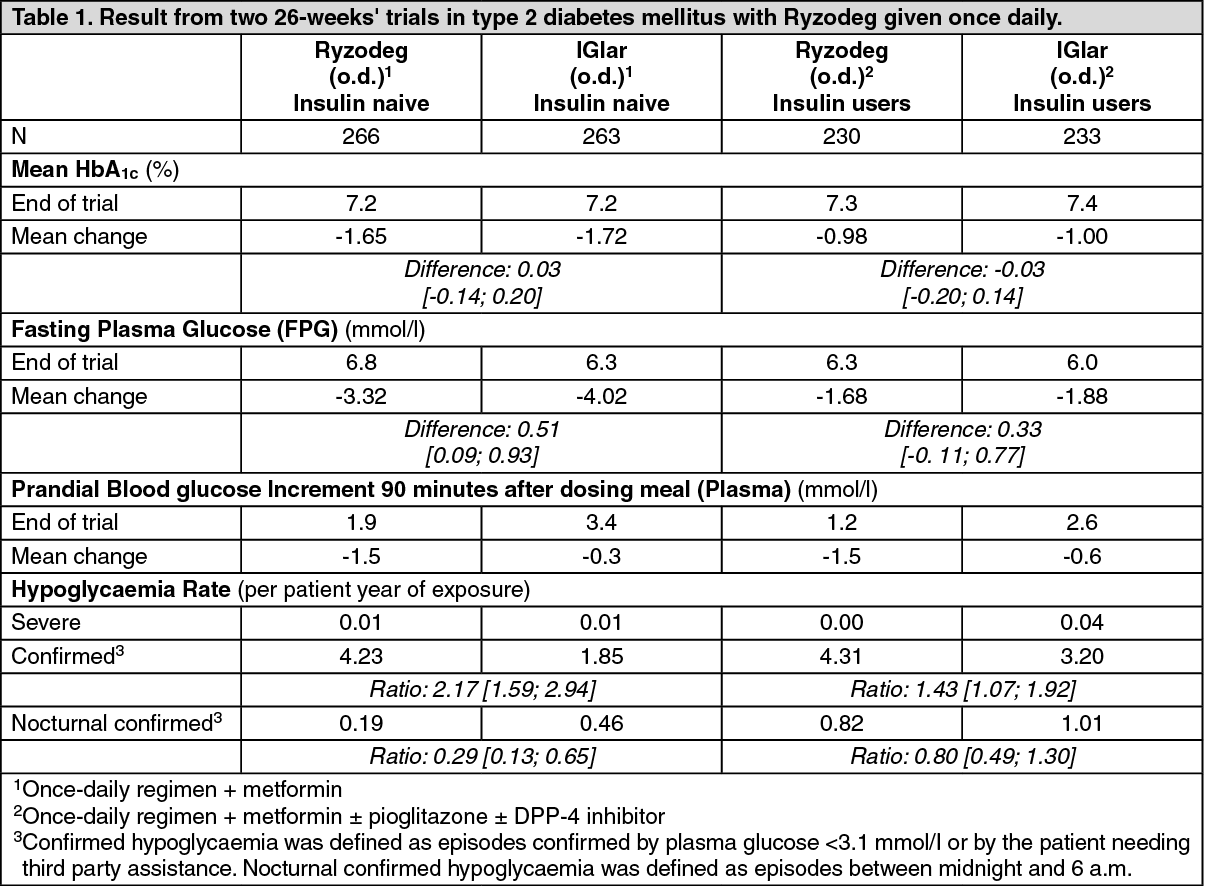
Clinical efficacy and safety: Five multi-national, randomised, controlled, open-label, treat-to-target clinical studies of 26 weeks' and 52 weeks' duration were conducted exposing a total of 1,360 patients with diabetes mellitus (362 patients in type 1 diabetes mellitus and 998 patients in type 2 diabetes mellitus) to Ryzodeg. Ryzodeg administered once daily (o.d.) plus Oral Antidiabetic Drugs (OADs) was compared to insulin glargine (IGlar) (o.d.) plus OADs in two trials in type 2 diabetes mellitus (Table 1). Ryzodeg b.i.d. plus OADs was compared to biphasic insulin aspart 30 (BIAsp 30) b.i.d. plus OADs in two trials in type 2 diabetes mellitus (Table 2). Ryzodeg o.d. plus insulin aspart (IAsp) was also compared to once-daily (o.d.) or twice-daily insulin detemir (IDet) plus IAsp in type 1 diabetes mellitus (Table 3).
Non-inferiority in HbA1c change from baseline to end-of-trial was confirmed in all studies against all comparators when treating patients to target.
In two trials combining insulin and OAD treatment in both insulin-naïve (insulin initiation) and insulin-using (insulin intensification) patients with type 2 diabetes mellitus, Ryzodeg o.d. demonstrated similar glycaemic control (HbA1c) compared to IGlar (administered according to label) (Table 1). As Ryzodeg contains a rapid-acting mealtime insulin (insulin aspart), prandial glycaemic control at the dosing meal is improved relative to administering basal insulin only; see trial results in Table 1. A lower rate of nocturnal hypoglycaemia (defined as episodes between midnight and 6 a.m. confirmed by plasma glucose < 3.1 mmol/l or by patient needing third party assistance) was observed with Ryzodeg relative to IGlar (Table 1).
Ryzodeg b.i.d. demonstrated similar glycaemic control (HbA1c) compared with BIAsp 30 b.i.d. in patients with type 2 diabetes mellitus. It demonstrates superior improvements in fasting plasma glucose levels compared to patients treated with BIAsp 30. Ryzodeg causes a lower rate of overall and nocturnal hypoglycaemia (Table 2).
In patients with type 1 diabetes mellitus, treatment with Ryzodeg o.d. plus IAsp for the remaining meals demonstrated similar glycaemic control (HbA1c and fasting plasma glucose) with a lower rate of nocturnal hypoglycaemia compared to a basal/bolus regimen with IDet plus IAsp at all meals (Table 3).
There is no clinically relevant development of insulin antibodies after long-term treatment of Ryzodeg. (See Tables 1, 2 and 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image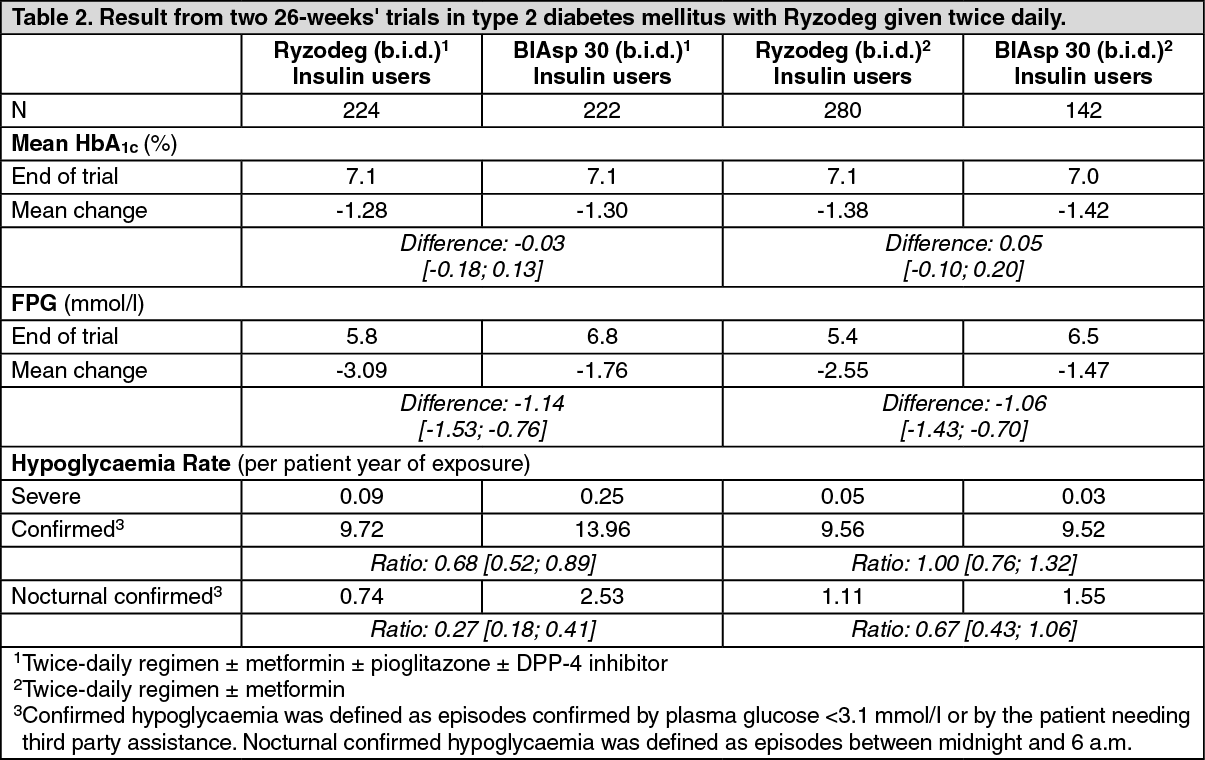 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePaediatric population: The efficacy and safety of Ryzodeg have been studied in a randomised controlled clinical trial in children and adolescents with diabetes mellitus type 1 for a period of 16 weeks (n=362). Patients in the Ryzodeg arm included 40 exposed children aged 2-5 years, 61 children aged 6-11 years and 80 adolescents aged 12-17 years. Ryzodeg dosed once daily with the main meal plus insulin aspart for the remaining meals showed similar reduction in HbA1c at week 16 and no differences in FPG and SMPG compared to comparator insulin detemir dosed once or twice daily plus mealtime insulin aspart. At week 16, the mean total daily insulin dose was 0.88 vs 1.01 units/kg in the Ryzodeg and insulin detemir arms, respectively. The rates (events per patient-year of exposure) of confirmed hypoglycaemia (ISPAD 2009 definition: 46.23 vs 49.55) and nocturnal confirmed hypoglycaemia (5.77 vs 5.40) were comparable with Ryzodeg versus insulin detemir whereas the rate of severe hypoglycaemia (0.26 vs 0.07) was higher in the Ryzodeg arm although the difference was not statistically significant. Few severe hypoglycaemic episodes were reported in each group; the observed rate of severe hypoglycaemia within the Ryzodeg arm was higher for subjects aged 2-5 years compared to subjects aged 6-11 years or 12-17 years (0.42 vs 0.21 and 0.21 respectively). An efficacy and safety evaluation for adolescent patients with type 2 diabetes mellitus has been made using data from adolescent and adult patients with type 1 diabetes mellitus and adult patients with type 2 diabetes mellitus. This assessment supports the use of Ryzodeg in adolescent patients with type 2 diabetes mellitus.
Pharmacokinetics: Absorption: After subcutaneous injection, soluble and stable multi-hexamers of insulin degludec are formed creating a depot of insulin in the subcutaneous tissue, while not interfering with the rapid release of insulin aspart monomers into the circulation. Insulin degludec monomers gradually separate from the multi-hexamers thus resulting in a slow and continuous delivery of insulin degludec into the circulation. Steady-state serum concentration of the basal component (insulin degludec) is reached after 2-3 days of daily Ryzodeg administration.
The rapid absorption characteristics of the well-established insulin aspart are maintained by Ryzodeg. The pharmacokinetic profile for insulin aspart appears 14 minutes after injection with a peak concentration after 72 minutes.
Distribution: The affinity of insulin degludec to serum albumin corresponds to a plasma protein binding of > 99% in human plasma. Insulin aspart has a low binding to plasma proteins (< 10%), similar to that seen with regular human insulin.
Biotransformation: Degradation of insulin degludec and insulin aspart is similar to that of human insulin; all metabolites formed are inactive.
Elimination: The half-life after subcutaneous administration of Ryzodeg is determined by the rate of absorption from the subcutaneous tissue. The half-life of the basal component (insulin degludec) at steady state is 25 hours independent of dose.
Linearity: Total exposure with Ryzodeg increases proportionally with increasing dose of the basal component (insulin degludec) and the mealtime component (insulin aspart) in type 1 and type 2 diabetes mellitus.
Gender: There is no gender difference in the pharmacokinetic properties of Ryzodeg.
Elderly, race, renal and hepatic impairment: There are no clinically relevant differences in the pharmacokinetics of Ryzodeg between elderly and younger adult patients, between races or between healthy subjects and patients with renal or hepatic impairment.
Paediatric population: The pharmacokinetic properties of Ryzodeg in type 1 diabetes mellitus were investigated in children (6-11 years) and adolescents (12-18 years) and compared to adults after single dose administration. The steady-state pharmacokinetic properties of the insulin degludec component of Ryzodeg were investigated using a population pharmacokinetic analysis in children down to 1 year of age.
Total exposure and peak concentration of insulin aspart were higher in children than in adults and were similar for adolescents and adults.
The pharmacokinetic properties of insulin degludec in children (1-11 years) and adolescents (12-18 years) were at steady state comparable to those observed in adults with type 1 diabetes mellitus. Total exposure of insulin degludec after single dose administration was, however, higher in children and adolescents than in adults with type 1 diabetes mellitus.
Toxicology: Preclinical safety data: Non-clinical data reveal no safety concerns for humans based on studies of safety pharmacology, repeated dose toxicity, carcinogenic potential, and toxicity to reproduction.
The ratio of mitogenic relative to metabolic potency for insulin degludec is comparable to that of human insulin.
Ryzodeg can be administered once or twice daily with the main meal(s). When needed, the patient can change the time of administration as long as Ryzodeg is dosed with the largest meal when taken once daily.
The potency of insulin analogues, including Ryzodeg, is expressed in units (U). One (1) unit (U) of Ryzodeg corresponds to 1 international unit (IU) of human insulin, 1 unit of insulin glargine, 1 unit of insulin detemir or 1 unit of biphasic insulin aspart.
In patients with type 2 diabetes mellitus, Ryzodeg can be administered alone, in combination with oral antidiabetic medicinal products, and in combination with bolus insulin (see Pharmacology: Pharmacodynamics under Actions).
In type 1 diabetes mellitus, Ryzodeg is combined with short-/rapid-acting insulin at the remaining meals.
Ryzodeg is to be dosed in accordance with the individual patient's needs. Dose-adjustments are recommended to be primarily based on fasting plasma glucose measurements.
As with all insulin products adjustment of dose may be necessary if patients undertake increased physical activity, change their usual diet or during concomitant illness.
Flexibility in dosing time: Ryzodeg allows for flexibility in the timing of insulin administration as long as it is dosed with the main meal(s).
If a dose of Ryzodeg is missed, the patient can take the missed dose with the next main meal of that day and thereafter resume the usual dosing schedule. Patients should not take an extra dose to make up for a missed dose.
Initiation: Patients with type 2 diabetes mellitus: The recommended total daily starting dose is 10 units with meal(s) followed by individual dosage adjustments.
Patients with type 1 diabetes mellitus: The recommended starting dose of Ryzodeg is 60-70% of the total daily insulin requirements.
Ryzodeg is to be used once daily at mealtime in combination with short-/rapid-acting insulin at the remaining meals followed by individual dosage adjustments.
Transfer from other insulin medicinal products: Close glucose monitoring is recommended during the transfer and in the following weeks. Doses and timing of concurrent rapid-acting or short-acting insulin products or other concomitant antidiabetic treatment may need to be adjusted.
Patients with type 2 diabetes mellitus: Patients switching from once-daily basal or premix insulin therapy can be converted unit-to-unit to once-daily Ryzodeg at the same total insulin dose as the patient's previous total daily insulin dose.
Patients switching from more than once-daily basal or premix insulin therapy can be converted unit-to-unit to twice-daily Ryzodeg at the same total insulin dose as the patient's previous total daily insulin dose.
Patients switching from basal/bolus insulin therapy to Ryzodeg will need to convert their dose based on individual needs. In general, patients are initiated on the same number of basal units.
Patients with type 1 diabetes mellitus: The recommended starting dose of Ryzodeg is 60-70% of the total daily insulin requirements in combination with short-/rapid-acting insulin at the remaining meals followed by individual dosage adjustments.
Special populations: Elderly (≥ 65 years old): Ryzodeg can be used in the elderly. Glucose monitoring is to be intensified and the insulin dose adjusted on an individual basis (see Pharmacology: Pharmacokinetics under Actions).
Renal and hepatic impairment: Ryzodeg can be used in renal and hepatic impaired patients. Glucose monitoring is to be intensified and the insulin dose adjusted on an individual basis (see Pharmacology: Pharmacokinetics under Actions).
Paediatric population: Ryzodeg can be used in adolescents and children from the age of 2 years (see Pharmacology: Pharmacodynamics under Actions). When changing from another insulin regimen to Ryzodeg, dose reduction of total insulin needs to be considered on an individual basis in order to minimise the risk of hypoglycaemia (see Precautions).
Ryzodeg should be used with special caution in children 2 to 5 years old because data from the clinical trial indicate that there may be a higher risk for severe hypoglycaemia in children in this age group (see Precautions, Adverse Reactions and Pharmacology: Pharmacodynamics under Actions).
Method of administration: Ryzodeg is for subcutaneous use only.
Ryzodeg must not be administered intravenously as it may result in severe hypoglycaemia.
Ryzodeg must not be administered intramuscularly as it may change the absorption.
Ryzodeg must not be used in insulin infusion pumps.
Ryzodeg must not be drawn from the cartridge of the pre-filled pen into a syringe (see Precautions).
Ryzodeg is administered subcutaneously by injection in the abdominal wall, the upper arm or the thigh. Injection sites are always to be rotated within the same region in order to reduce the risk of lipodystrophy.
Patients should be instructed to always use a new needle. The re-use of insulin pen needles increases the risk of blocked needles, which may cause under- or overdosing. In the event of blocked needles, patients must follow the instructions described in the instructions for use accompanying this leaflet (see Special precautions for disposal and other handling under Cautions for Usage).
Ryzodeg comes in a pre-filled pen (FlexTouch) designed to be used with NovoFine or NovoTwist injection needles. The pre-filled pen delivers 1-80 units in steps of 1 unit.
Mild hypoglycaemic episodes can be treated by oral administration of glucose or other products containing sugar. It is therefore recommended that the patient always carries glucose-containing products.
Severe hypoglycaemic episodes, where the patient is not able to treat himself, can be treated with glucagon (0.5 to 1 mg) given intramuscularly or subcutaneously by a trained person, or with glucose given intravenously by a healthcare professional. Glucose must be given intravenously if the patient does not respond to glucagon within 10 to 15 minutes. Upon regaining consciousness, administration of oral carbohydrates is recommended for the patient in order to prevent a relapse.
Hypoglycaemia may occur if the insulin dose is too high in relation to the insulin requirement.
In children, extra care should be taken to match insulin doses with food intake and physical activities in order to minimise the risk of hypoglycaemia. Ryzodeg may be associated with higher occurrence of severe hypoglycaemia compared to a basal-bolus regimen in the paediatric population, particularly in children 2 to 5 years old (see Pharmacology: Pharmacodynamics under Actions). For this age group, Ryzodeg should be considered on an individual basis.
Patients whose blood glucose control is greatly improved (e.g. by intensified insulin therapy) may experience a change in their usual warning symptoms of hypoglycaemia and must be advised accordingly. Usual warning symptoms may disappear in patients with long-standing diabetes.
Concomitant illness, especially infections and fever, usually increases the patient's insulin requirement. Concomitant diseases in the kidney, liver or diseases affecting the adrenal, pituitary or thyroid gland may require changes in the insulin dose.
As with other basal insulin products or insulin products with a basal component, the prolonged effect of Ryzodeg may delay recovery from hypoglycaemia.
Hyperglycaemia: Administration of rapid-acting insulin is recommended in situations with severe hyperglycaemia.
Inadequate dosing and/or discontinuation of treatment in patients requiring insulin may lead to hyperglycaemia and potentially to diabetic ketoacidosis. Furthermore, concomitant illness, especially infections, may lead to hyperglycaemia and thereby cause an increased insulin requirement.
Usually, the first symptoms of hyperglycaemia develop gradually over a period of hours or days. They include thirst, increased frequency of urination, nausea, vomiting, drowsiness, flushed dry skin, dry mouth, and loss of appetite as well as acetone odour of breath. In type 1 diabetes mellitus, untreated hyperglycaemic events eventually lead to diabetic ketoacidosis, which is potentially lethal.
Transfer from other insulin medicinal products: Transferring a patient to another type, brand or manufacturer of insulin must be done under medical supervision and may result in the need for a change in dosage.
Combination of thiazolidinediones and insulin medicinal products: Cases of cardiac failure have been reported when thiazolidinediones were used in combination with insulin, especially in patients with risk factors for development of cardiac failure. This should be kept in mind if treatment with the combination of thiazolidinediones and Ryzodeg is considered. If the combination is used, patients should be observed for signs and symptoms of heart failure, weight gain and oedema. Thiazolidinediones should be discontinued if any deterioration in cardiac symptoms occurs.
Eye disorder: Intensification of insulin therapy with abrupt improvement in glycaemic control may be associated with temporary worsening of diabetic retinopathy, while long-term improved glycaemic control decreases the risk of progression of diabetic retinopathy.
Avoidance of accidental mix-ups: Patients must be instructed to always check the insulin label before each injection to avoid accidental mix-ups between Ryzodeg and other insulin products.
Patients must visually verify the dialled units on the dose counter of the pen. Therefore, the requirement for patients to self-inject is that they can read the dose counter on the pen. Patients who are blind or have poor vision must be instructed to always get help/assistance from another person who has good vision and is trained in using the insulin device.
To avoid dosing errors and potential overdose, patients and healthcare professionals should never use a syringe to draw the medicinal product from the cartridge in the pre-filled pen.
In the event of blocked needles, patients must follow the instructions described in the instructions for use accompanying this leaflet (see Special precautions for disposal and other handling under Cautions for Usage).
Insulin antibodies: Insulin administration may cause insulin antibodies to form. In rare cases, the presence of such insulin antibodies may necessitate adjustment of the insulin dose in order to correct a tendency to hyper- or hypoglycaemia.
Effects on ability to drive and use machines: The patient's ability to concentrate and react may be impaired as a result of hypoglycaemia. This may constitute a risk in situations where these abilities are of special importance (e.g. driving a car or using machines).
Patients must be advised to take precautions to avoid hypoglycaemia while driving. This is particularly important in those who have reduced or absent awareness of the warning signs of hypoglycaemia or have frequent episodes of hypoglycaemia. The advisability of driving should be considered in these circumstances.
Animal reproduction studies have not revealed any difference between insulin degludec and human insulin regarding embryotoxicity and teratogenicity.
In general, intensified blood glucose control and monitoring of pregnant women with diabetes are recommended throughout pregnancy and when contemplating pregnancy. Insulin requirements usually decrease in the first trimester and increase subsequently during the second and third trimesters. After delivery, insulin requirements usually return rapidly to pre-pregnancy values.
Breast-feeding: There is no clinical experience with Ryzodeg during breast-feeding. In rats, insulin degludec was secreted in milk; the concentration in milk was lower than in plasma.
It is unknown whether insulin degludec/insulin aspart is excreted in human milk. No metabolic effects are anticipated in the breast-fed newborn/infant.
Fertility: Animal reproduction studies with insulin degludec have not revealed any adverse effects on fertility.
Tabulated list of adverse reactions: Adverse reactions listed as follows are based on clinical trial data and classified according to MedDRA System Organ Class. Frequency categories are defined according to the following convention: Very common (≥ 1/10); common (≥ 1/100 to < 1/10); uncommon (≥ 1/1,000 to < 1/100); rare (≥ 1/10,000 to < 1/1,000); very rare (< 1/10,000) and not known (cannot be estimated from the available data). (See Table 4.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDescription of selected adverse reactions: Immune system disorders: With insulin preparations, allergic reactions may occur. Immediate-type allergic reactions to either insulin itself or the excipients may potentially be life-threatening.
With Ryzodeg, hypersensitivity (manifested with swelling of tongue and lips, diarrhoea, nausea, tiredness and itching) and urticaria were reported rarely.
Hypoglycaemia: Hypoglycaemia may occur if the insulin dose is too high in relation to the insulin requirement. Severe hypoglycaemia may lead to unconsciousness and/or convulsions and may result in temporary or permanent impairment of brain function or even death. The symptoms of hypoglycaemia usually occur suddenly. They may include cold sweats, cool pale skin, fatigue, nervousness or tremor, anxiousness, unusual tiredness or weakness, confusion, difficulty in concentration, drowsiness, excessive hunger, vision changes, headache, nausea and palpitation.
Lipodystrophy: Lipodystrophy (including lipohypertrophy, lipoatrophy) may occur at the injection site. Continuous rotation of the injection site within the particular injection area may help to reduce the risk of developing these reactions.
Injection site reactions: Injection site reactions (including injection site haematoma, pain, haemorrhage, erythema, nodules, swelling, discolouration, pruritus, warmth and injection site mass) occurred in patients treated with Ryzodeg. These reactions are usually mild and transitory and they normally disappear during continued treatment.
Paediatric population: Ryzodeg has been administered to children and adolescents up to 18 years of age for the investigation of pharmacokinetic properties (see Pharmacology: Pharmacokinetics under Actions). Safety and efficacy have been demonstrated in a trial in children aged 2 to less than 18 years. The frequency, type and severity of adverse reactions in the paediatric population do not indicate differences to the experience in the general diabetes population with the exception of a signal of higher occurrence of severe hypoglycaemia compared to a basal-bolus regimen in the paediatric population, particularly in children 2 to 5 years old (see Dosage & Administration, Precautions and Pharmacology: Pharmacodynamics under Actions).
Other special populations: Based on results from clinical trials, the frequency, type and severity of adverse reactions observed in the elderly and in patients with renal or hepatic impairment do not indicate any differences to the broader experience in the general population.
The following substances may reduce the insulin requirement: Oral antidiabetic medicinal products, GLP-1 receptor agonists, monoamine oxidase inhibitors (MAOI), beta-blockers, angiotensin converting enzyme (ACE) inhibitors, salicylates, anabolic steroids and sulfonamides.
The following substances may increase the insulin requirement: Oral contraceptives, thiazides, glucocorticoids, thyroid hormones, sympathomimetics, growth hormone and danazol.
Beta-blockers may mask the symptoms of hypoglycaemia.
Octreotide/lanreotide may either increase or decrease the insulin requirement.
Alcohol may intensify or reduce the hypoglycaemic effect of insulin.
Ryzodeg must not be used if the solution does not appear clear and colourless.
Ryzodeg which has been frozen must not be used.
A new needle must always be attached before each use. Needles must not be re-used. The patient should discard the needle after each injection.
In the event of blocked needles, patients must follow the instructions described in the instructions for use, see Patient Counselling Information.
Any waste material should be disposed of in accordance with local requirements.
The pre-filled pen (FlexTouch) is designed to be used with NovoFine/NovoTwist injection needles up to a length of 8 mm. It delivers 1-80 units in steps of 1 unit.
For detailed instructions for use, see Patient Counselling Information.
Incompatibilities: Substances added to Ryzodeg may cause degradation of insulin degludec and/or insulin aspart.
Ryzodeg must not be added to infusion fluids.
This medicinal product must not be mixed with any other product.
Do not freeze.
Keep the cap on the pen in order to protect from light.
After first opening or carried as a spare: The product may be stored for a maximum of 4 weeks. Do not store above 30°C. Can be stored in a refrigerator (2°C - 8°C). Keep the cap on the pen in order to protect from light.
If you do not follow the instructions carefully, you may get too little or too much insulin, which can lead to too high or too low blood sugar level.
Do not use the pen without proper training from your doctor or nurse.
Start by checking your pen to make sure that it contains Ryzodeg 100 units/ml.
If you are blind or have poor eyesight and cannot read the dose counter on the pen, do not use this pen without help. Get help from a person with good eyesight who is trained to use the FlexTouch pre-filled pen.
Your pen is a pre-filled dial-a-dose insulin pen containing 300 units of insulin. You can select a maximum of 80 units per dose, in steps of 1 unit. Your pen is designed to be used with NovoTwist or NovoFine single-use disposable needles up to a length of 8 mm. Needles are not included in the pack.
Prepare your pen: Check the name and strength on the label of your pen, to make sure that it contains Ryzodeg 100 units/ml. This is especially important if you take more than one type of insulin. If you take a wrong type of insulin, your blood sugar level may get too high or too low.
Pull off the pen cap.
Check that the insulin in your pen is clear and colourless. Look through the insulin window. If the insulin looks cloudy, do not use the pen.
Take a new needle and tear off the paper tab.
Push the needle straight onto the pen. Turn until it is on tight.
Pull off the outer needle cap and keep it for later. You will need it after the injection, to correctly remove the needle from the pen.
Pull off the inner needle cap and throw it away. If you try to put it back on, you may accidentally stick yourself with the needle.
A drop of insulin may appear at the needle tip. This is normal, but you must still check the insulin flow.
Always use a new needle for each injection. This reduces the risk of contamination, infection, leakage of insulin, blocked needles and inaccurate dosing.
Never use a bent or damaged needle.
Check the insulin flow: Always check the insulin flow before you start. This helps you to ensure that you get your full insulin dose.
Turn the dose selector to select 2 units. Make sure the dose counter shows 2.
Hold the pen with the needle pointing up.
Tap the top of the pen gently a few times to let any air bubbles rise to the top.
Press and hold in the dose button until the dose counter returns to 0.
The 0 must line up with the dose pointer.
A drop of insulin should appear at the needle tip.
A small air bubble may remain at the needle tip, but it will not be injected.
If no drop appears, repeat the steps up to 6 times. If there is still no drop, change the needle and repeat the steps once more.
If a drop of insulin still does not appear, dispose of the pen and use a new one.
Always make sure that a drop appears at the needle tip before you inject. This makes sure that the insulin flows. If no drop appears, you will not inject any insulin, even though the dose counter may move.
This may indicate a blocked or damaged needle.
Always check the flow before you inject. If you do not check the flow, you may get too little insulin or no insulin at all. This may lead to too high blood sugar level.
Select your dose: Make sure the dose counter shows 0 before you start.
The 0 must line up with the dose pointer.
Turn the dose selector to select the dose you need, as directed by your doctor or nurse.
If you select a wrong dose, you can turn the dose selector forwards or backwards to the correct dose.
The pen can dial up to a maximum of 80 units.
The dose selector changes the number of units. Only the dose counter and dose pointer will show how many units you select per dose.
You can select up to 80 units per dose. When your pen contains less than 80 units, the dose counter stops at the number of units left.
The dose selector clicks differently when turned forwards, backwards or past the number of units left. Do not count the pen clicks.
Always use the dose counter and the dose pointer to see how many units you have selected before injecting the insulin.
Do not count the pen clicks. If you select and inject the wrong dose, your blood sugar level may get too high or too low. Do not use the insulin scale, it only shows approximately how much insulin is left in your pen.
Inject your dose: Insert the needle into your skin as your doctor or nurse has shown you.
Make sure you can see the dose counter.
Do not touch the dose counter with your fingers. This could interrupt the injection.
Press and hold down the dose button until the dose counter returns to 0.
The 0 must line up with the dose pointer.
You may then hear or feel a click.
Leave the needle under the skin for at least 6 seconds to make sure you get your full dose.
Pull the needle and pen straight up from your skin.
If blood appears at the injection site, press lightly with a cotton swab. Do not rub the area.
You may see a drop of insulin at the needle tip after injecting. This is normal and does not affect your dose.
Always watch the dose counter to know how many units you inject.
The dose counter will show the exact number of units. Do not count the pen clicks.
Hold the dose button down until the dose counter returns to 0 after the injection. If the dose counter stops before it returns to 0, the full dose has not been delivered, which may result in too high blood sugar level.
After your injection: Lead the needle tip into the outer needle cap on a flat surface without touching the needle or the outer cap.
Once the needle is covered, carefully push the outer needle cap completely on.
Unscrew the needle and dispose of it carefully.
Put the pen cap on your pen after each use to protect the insulin from light.
Always dispose of the needle after each injection. This reduces the risk of contamination, infection, leakage of insulin, blocked needles and inaccurate dosing. If the needle is blocked, you will not inject any insulin.
When the pen is empty, throw it away without a needle on as instructed by your doctor, nurse, pharmacist or local authorities.
Never try to put the inner needle cap back on the needle. You may stick yourself with the needle.
Always remove the needle after each injection and store your pen without the needle attached. This reduces the risk of contamination, infection, leakage of insulin, blocked needles and inaccurate dosing.
How much insulin is left?: The insulin scale shows you approximately how much insulin is left in your pen.
To see precisely how much insulin is left, use the dose counter: Turn the dose selector until the dose counter stops. If it shows 80, at least 80 units are left in your pen.
If it shows less than 80, the number shown is the number of units left in your pen.
Turn the dose selector back until the dose counter shows 0.
If you need more insulin than the units left in your pen, you can split your dose between two pens.
Be very careful to calculate correctly if splitting your dose.
If in doubt, take the full dose with a new pen. If you split the dose wrong, you will inject too little or too much insulin, which can lead to too high or too low blood sugar level.
Further important information: Always keep your pen with you.
Always carry an extra pen and new needles with you, in case of loss or damage.
Always keep your pen and needles out of sight and reach of others, especially children.
Never share your pen or your needles with other people. It might lead to cross-infection.
Never share your pen with other people. Your medicine might be harmful to their health.
Caregivers must be very careful when handling used needles - to reduce the risk of needle injury and cross-infection.
Caring for your pen: Treat your pen with care. Rough handling or misuse may cause inaccurate dosing, which can lead to too high or too low blood sugar level.
Do not leave the pen in a car or other place where it can get too hot or too cold.
Do not expose your pen to dust, dirt or liquid.
Do not wash, soak or lubricate your pen. If necessary, clean it with mild detergent on a moistened cloth.
Do not drop your pen or knock it against hard surfaces.
If you drop it or suspect a problem, attach a new needle and check the insulin flow before you inject.
Do not try to refill your pen. Once empty, it must be disposed of.
Do not try to repair your pen or pull it apart.
Frequently Bought Products
-
৳1,030.00
৳1,550.00 -
৳250.00
৳500.00 -
৳110.00
৳150.00 -
৳12.00
৳15.00 -
৳775.60
৳1,108.00 -
৳130.00
৳135.00
মজুমদার শপ - MShopBD | Trusted Online Shop in Bangladesh
MShopBD (মজুমদার শপ) is a leading and trusted online shopping platform in Bangladesh. আমরা সাশ্রয়ী মূল্যে ১০০% জেনুইন ফ্যাশন, গ্যাজেট, গ্রোসারি এবং প্রিমিয়াম কোয়ালিটির হার্বাল ও অর্গানিক পণ্য সরবরাহ করি। Shop with confidence at MShopBD for the best online shopping experience with fast home delivery, secure payments, and authentic products across BD. মজুমদার শপ - স্মার্ট শপিং এখন আপনার হাতের মুঠোয়। Legal Credentials:: ESDP ( esdp.gov.bd) Reg No: 355611/2021,BSCIC Reg No: GO-20260208-0024063, BSCIC Trade No: TR-202604000152.
MShopBD (মজুমদার শপ) বাংলাদেশের একটি বিশ্বস্ত এবং জনপ্রিয় ই-কমার্স প্ল্যাটফর্ম। আমরা সাশ্রয়ী মূল্যে ১০০% কোয়ালিটিসম্পন্ন ফ্যাশন, লাইফস্টাইল, ইলেকট্রনিক্স এবং প্রিমিয়াম হার্বাল ও ন্যাচারাল পণ্য সরাসরি আপনার দোরগোড়ায় পৌঁছে দেই। গ্রাহকের সন্তুষ্টি ও পণ্যের গুণগত মান বজায় রাখাই আমাদের প্রধান লক্ষ্য। Fast Home Delivery, Secure Payments এবং Authentic Products-এর নিশ্চয়তা নিয়ে MShopBD এখন আপনার স্মার্ট শপিং পার্টনার।
